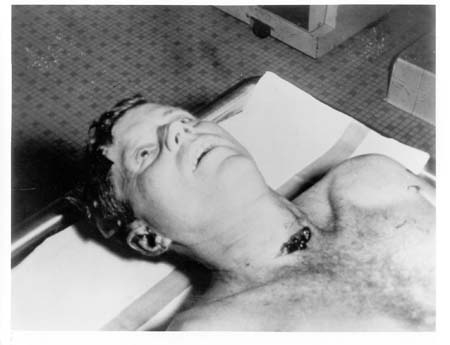
Autopsy Photos taken at Bethesda
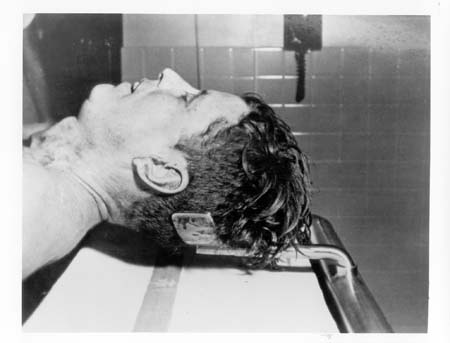
Side view

Top view
Front view

Side-on back view

Full back view

Colour photo
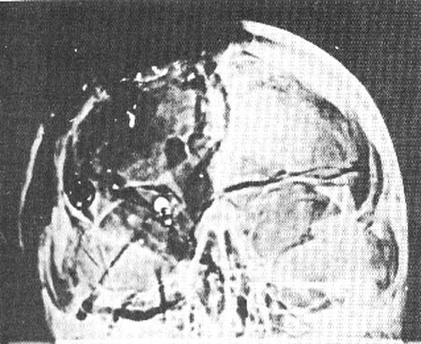
X-Ray of Kennedy's skull
Autopsy Report
Date 11/22/63 1300 (CST)
Prosecter: CDR J.J. Humes, MC, USA (497831)
Assistant: CDR "J" Thornton Boswell, MC, USN, (439878); LCOL, Pierre A. Finck, MC, USA (04 043 322)
Full Autopsy
Ht. - 72 1/2 inches Wt. - 170 pounds Eyes - blue Hair - Reddish brown
Pathological diagnosis: Cause of Death: Gunshot wound, head.
Signature: J.J. Humes, CDS, MC, USN
Military organization: President, United States
Age: 46 Sex: Male Race: Caucasian
Autopsy No. A63-272
Patient's Identification: Kennedy, John F., Naval Medical School
Clinical Summary
According to available information the deceased, President John F. Kennedy, was riding in an open car in a motorcade during an official visit to Dallas, Texas on 22 November 1963. The President was sitting in the right rear seat with Mrs. Kennedy seated on the same seat to his left. Sitting directly in front of the President was Governor John B. Connally of Texas and directly in front of Mrs. Kennedy sat Mrs. Connally. The vehicle was moving at a slow rate of speed down an incline into an underpass that leads to a freeway route to the Dallas Trade Mart where the President was to deliver an address.
Three shots were heard and the President fell forward bleeding from the head. (Governor Connally was seriously wounded by the same gunfire.) According to newspaper reports ("Washington Post" November 23, 1963) Bob Jackson, a Dallas "Times Herald" Photographer, said he looked around as he heard the shots and saw a rifle barrel disappearing into a window on an upper floor of the nearby Texas School Book Depository Building.
Shortly following the wounding of the two men the car was driven to Parkland Hospital in Dallas. In the emergency room of that hospital the President was attended by Dr. Malcolm Perry. Telephone communication with Dr. Perry on November 23, 1963 develops the following information relative to the observations made by Dr. Perry and procedures performed there prior to death.
Dr. Perry noted the massive wound of the head and a second much smaller wound of the low anterior neck in approximately the midline. A tracheostomy was performed by extending the latter wound. At this point bloody air was noted bubbling from the wound and an injury to the right lateral wall of the trachea was observed. Incisions were made in the upper anterior chest wall bilaterally to combat possible subcutaneous emphysema. Intravenous infusions of blood and saline were begun and oxygen was administered. Despite these measures cardiac arrest occurred and closed chest cardiac massage failed to re-establish cardiac action. The President was pronounced dead approximately thirty to forty minutes after receiving his wounds.
The remains were transported via the Presidential plane to Washington, D.C. and subsequently to the Naval Medical School, National Naval Medical Center, Bethesda, Maryland for postmortem examination.
General Description of the Body
The body is that of a muscular, well-developed and well nourished adult Caucasian male measuring 72 1/2 inches and weighing approximately 170 pounds. There is beginning rigor mortis, minimal dependent livor mortis of the dorsum, and early algor mortis. The hair is reddish brown and abundant, the eyes are blue, the right pupil measuring 8 mm. in diameter, the left 4 mm. There is edema and ecchymosis of the inner canthus region of the left eyelid measuring approximately 1.5 cm. in greatest diameter. There is edema and ecchymosis diffusely over the right supra-orbital ridge with abnormal mobility of the underlying bone. (The remainder of the scalp will be described with the skull.) There is clotted blood on the external ears but otherwise the ears, nares, and mouth are essentially unremarkable. The teeth are in excellent repair and there is some pallor of the oral mucous membrane.
Situated on the upper right posterior thorax just above the upper border of the scapula there is a 7 x 4 millimeter oval wound. This wound is measured to be 14 cm. from the tip of the right acromion process and 14 cm. below the tip of the right mastoid process.
Situated in the low anterior neck at approximately the level of the third and fourth tracheal rings is a 6.5 cm. long transverse wound with widely gaping irregular edges. (The depth and character of these wounds will be further described below.)
Situated on the anterior chest wall in the nipple line are bilateral 2 cm. long recent transverse surgical incisions into the subcutaneous tissue. The one on the left is situated 11 cm. cephalad to the nipple and the one on the right 8 cm. cephalad to the nipple. There is no hemorrhage or ecchymosis associated with these wounds. A similar clean wound measuring 2 cm. in length is situated on the antero-lateral aspect of the left mid arm. Situated on the antero-lateral aspect of each ankle is a recent 2 cm. transverse incision into the subcutaneous tissue.
There is an old well healed 8 cm. McBurney abdominal incision. Over the lumbar spine in the midline is an old, well healed 15 cm. scar. Situated on the upper antero-lateral aspect of the right thigh is an old, well healed 8 cm. scar.
Missile Wounds
1. There is a large irregular defect of the scalp and skull on the right involving chiefly the parietal bone but extending somewhat into the temporal and occipital regions. In this region there is an actual absence of scalp and bone producing a defect which measures approximately 13 cm. in greatest diameter.
From the irregular margins of the above scalp defect tears extend in stellate fashion into the more or less intact scalp as follows:
a. From the right inferior temporo-parietal margin anterior to the right ear to a point slightly above the tragus.
b. From the anterior parietal margin anteriorly on the forehead to approximately 4 cm. above the right orbital ridge.
c. From the left margin of the main defect across the midline antero-laterally for a distance of approximately 8 cm.
d. From the same starting point as c. 10 cm. postero-laterally.
Situated in the posterior scalp approximately 2.5 cm. laterally to the right and slightly above the external occipital protuberance is a lacerated wound measuring 15 x 6 mm. In the underlying bone is a corresponding wound through the skull which exhibits beveling of the margins of the bone when viewed from the inner aspect of the skull.
Clearly visible in the above described large skull defect and exuding from it is lacerated brain tissue which on close inspection proves to represent the major portion of the right cerebral hemisphere. At this point it is noted that the falx cerebri is extensively lacerated with disruption of the superior saggital sinus.
Upon reflecting the scalp multiple complete fracture lines are seen to radiate from both the large defect at the vertex and the smaller wound at the occiput. These vary greatly in length and direction, the longest measuring approximately 19 cm. These result in the production of numerous fragments which vary in size from a few millimeters to 10 cm. in greatest diameter.
The complexity of these fractures and the fragments thus produced tax satisfactory verbal description and are better appreciated in photographs and roentgenograms which are prepared.
The brain is removed and preserved for further study following formal in fixation.
Received as separate specimens from Dallas, Texas are three fragments of skull bone which in aggregate roughly approximate the dimensions of the large defect described above. At one angle of the largest of these fragments is a portion of the perimeter of a roughly circular wound presumably of exit which exhibits beveling of the outer aspect of the bone and is estimated to measure approximately 2.5 to 3.0 cm. in diameter. Roentgenograms of this fragment reveal minute particles of metal in the bone at this margin. Roentgenograms of the skull reveal multiple minute metallic fragments along a line corresponding with a line joining the above described small occipital wound and the right supra-orbital ridge. From the surface of the disrupted right cerebral cortex two small irregularly shaped fragments of metal are recovered. These measure 7 x 2 mm. and 3 x 1 mm. These are placed in the custody of Agents Francis X. O'Neill, Jr. and James W. Sibert, of the Federal Bureau of Investigation, who executed a receipt therefore (attached).
2. The second wound presumably of entry is that described above in the upper right posterior thorax. Beneath the skin there is ecchymosis of subcutaneous tissue and musculature. The missile path through the fascia and musculature cannot be easily proved. The wound presumably of exit was that described by Dr. Malcolm Perry of Dallas in the low anterior cervical region. When observed by Dr. Perry the wound measured "a few millimeters in diameter", however it was extended as a tracheostomy incision and thus its character is distorted at the time of autopsy. However there is considerable eccymosis of the strap muscles of the right side of the neck and of the fascia about the trachea adjacent to the line of the tracheostomy wound. The third point of reference in connecting these two wounds is in the apex (supra-clavicular portion) of the right pleural cavity. In this region there is contusion of the parietal pleura and of the extreme apical portion of the right upper lobe of the lung. In both instances the diameter of contusion and ecchymosis at the point of maximal involvement measures 5 cm. Both the visceral and parietal pleura are intact overlying these areas of trauma.
Incisions
The scalp wounds are extended in the coronal plane to examine the cranial content and the customary (Y) shaped incision is used to examine the body cavities.
Skeletal System
Aside from the above described skull wounds there are no significant gross skeletal abnormalities.
Photography
Black and white and color photographs depicting significant findings are exposed but not developed. These photographs were placed in the custody of Agent Roy E. Kellerman of the U.S. Secret Service, who executed a receipt therefore (attached).
Roentgenograms
Roentgenograms are made of the entire body and of the separately submitted three fragments of skull bone. These are developed are were placed in the custody of Agent Roy H. Kellerman of the U.S. Secret Service, who executed a receipt therefore (attached).
Summary
Based on the above observations it is our opinion that the deceased died as a result of two perforating gunshot wounds inflicted by high velocity projectiles fired by a person or persons unknown. The projectiles were fired from a point behind and somewhat above the level of the deceased. The observations and available information do not permit a satisfactory estimate as to the sequence of the two wounds.
The fatal missile entered the skull above and to the right of the external occipital protuberance. A portion of the projectile traversed the cranial cavity in a posterior-anterior direction (see lateral skull roentgenograms) depositing minute particles along its path. A portion of the projectile made its exit through the parietal bone on the right carrying with it portions of cerebrum, skull and scalp. The two wounds of the skull combined with the force of the missile produced extensive fragmentation of the skull, laceration of the superior saggital sinus, and of the right cerebral hemisphere.
The other missile entered the right superior posterior thorax above the scapula and traversed the soft tissues of the supra-scapular and the supra-clavicular portions of the base of the right side of the neck. This missile produced contusions of the right apical parietal pleura and of the apical portion of the right upper lobe of the lung. The missile contused the strap muscles of the right side of the neck, damaged the trachea and made its exit through the anterior surface of the neck. As far as can be ascertained this missile struck no bony structures in its path through the body.
In addition, it is our opinion that the wound of the skull produced such extensive damage to the brain as to preclude the possibility of the deceased surviving this injury.
A supplementary report will be submitted following more detailed examination of the brain and of microscopic sections. However, it is not anticipated that these examinations will materially alter the findings.
Supplementary Report of Autopsy Number A63-272 President John F. Kennedy
Pathological Examination Report No. A63-272
Gross Description of the Brain
Following formalin fixation the brain weighs 1500 gms. The right cerebral hemisphere is found to be markedly disrupted. There is a longitudinal laceration of the right hemisphere which is para-sagittal in position approximately 2.5 cm. to the right of the of the midline which extends from the tip of the occipital lobe posteriorly to the tip of the frontal lobe anteriorly. The base of the laceration is situated approximately 4.5 cm. below the vertex in the white matter. There is considerable loss of cortical substance above the base of the laceration, particularly in the parietal lobe. The margins of this laceration are at all points jagged and irregular, with additional lacerations extending in varying directions and for varying distances from the main laceration. In addition, there is a laceration of the corpus callosum extending from the genu to the tail. Exposed in this latter laceration are the interiors of the right lateral and third ventricles.
When viewed from the vertex the left cerebral hemisphere is intact. There is marked engorgement of meningeal blood vessels of the left temporal and frontal regions with considerable associated sub-arachnoid hemorrhage. The gyri and sulci over the left hemisphere are of essentially normal size and distribution. Those on the right are too fragmented and distorted for satisfactory description.
When viewed from the basilar aspect the disruption of the right cortex is again obvious. There is a longitudinal laceration of the mid-brain through the floor of the third ventricle just behind the optic chiasm and the mammillary bodies. This laceration partially communicates with an oblique 1.5 cm. tear through the left cerebral peduncle. There are irregular superficial lacerations over the basilar aspects of the left temporal and frontal lobes.
In the interest of preserving the specimen coronal sections are not made. The following sections are taken for microscopic examination:
a. From the margin of the laceration in the right parietal lobe.
b. From the margin of the laceration in the corpus callosum.
c. From the anterior portion of the laceration in the right frontal lobe.
d. From the contused left fronto-parietal cortex.
e. From the line of transection of the spinal cord.
f. From the right cerebellar cortex.
g. From the superficial laceration of the basilar aspect of the left temporal lobe.
During the course of this examination seven (7) black and white and six (6) color 4x5 inch negatives are exposed but not developed (the cassettes containing these negatives have been delivered by hand to Rear Admiral George W. Burkley, MC, USN, White House Physician).
Microscopic Examination
Brain
Multiple sections from representative areas as noted above are examined. All sections are essentially similar and show extensive disruption of brain tissue with associated hemorrhage. In none of the sections examined are there significant abnormalities other than those directly related to the recent trauma.
Skin Wounds
Sections through the wounds in the occipital and upper right posterior thoracic regions are essentially similar. In each there is loss of continuity of the epidermis with coagulation necrosis of the tissues at the wound margins. The scalp wound exhibits several small fragments of bone at its margins in the subcutaneous tissue.
Final Summary
This supplementary report covers in more detail the extensive degree of cerebral trauma in this case. However neither this portion of the examination nor the microscopic examinations alter the previously submitted report or add significant details to the cause of death.
/s/
J. J. HUMES
CDR, MC, USN, 497831
Prosecter: CDR J.J. Humes, MC, USA (497831)
Assistant: CDR "J" Thornton Boswell, MC, USN, (439878); LCOL, Pierre A. Finck, MC, USA (04 043 322)
Full Autopsy
Ht. - 72 1/2 inches Wt. - 170 pounds Eyes - blue Hair - Reddish brown
Pathological diagnosis: Cause of Death: Gunshot wound, head.
Signature: J.J. Humes, CDS, MC, USN
Military organization: President, United States
Age: 46 Sex: Male Race: Caucasian
Autopsy No. A63-272
Patient's Identification: Kennedy, John F., Naval Medical School
Clinical Summary
According to available information the deceased, President John F. Kennedy, was riding in an open car in a motorcade during an official visit to Dallas, Texas on 22 November 1963. The President was sitting in the right rear seat with Mrs. Kennedy seated on the same seat to his left. Sitting directly in front of the President was Governor John B. Connally of Texas and directly in front of Mrs. Kennedy sat Mrs. Connally. The vehicle was moving at a slow rate of speed down an incline into an underpass that leads to a freeway route to the Dallas Trade Mart where the President was to deliver an address.
Three shots were heard and the President fell forward bleeding from the head. (Governor Connally was seriously wounded by the same gunfire.) According to newspaper reports ("Washington Post" November 23, 1963) Bob Jackson, a Dallas "Times Herald" Photographer, said he looked around as he heard the shots and saw a rifle barrel disappearing into a window on an upper floor of the nearby Texas School Book Depository Building.
Shortly following the wounding of the two men the car was driven to Parkland Hospital in Dallas. In the emergency room of that hospital the President was attended by Dr. Malcolm Perry. Telephone communication with Dr. Perry on November 23, 1963 develops the following information relative to the observations made by Dr. Perry and procedures performed there prior to death.
Dr. Perry noted the massive wound of the head and a second much smaller wound of the low anterior neck in approximately the midline. A tracheostomy was performed by extending the latter wound. At this point bloody air was noted bubbling from the wound and an injury to the right lateral wall of the trachea was observed. Incisions were made in the upper anterior chest wall bilaterally to combat possible subcutaneous emphysema. Intravenous infusions of blood and saline were begun and oxygen was administered. Despite these measures cardiac arrest occurred and closed chest cardiac massage failed to re-establish cardiac action. The President was pronounced dead approximately thirty to forty minutes after receiving his wounds.
The remains were transported via the Presidential plane to Washington, D.C. and subsequently to the Naval Medical School, National Naval Medical Center, Bethesda, Maryland for postmortem examination.
General Description of the Body
The body is that of a muscular, well-developed and well nourished adult Caucasian male measuring 72 1/2 inches and weighing approximately 170 pounds. There is beginning rigor mortis, minimal dependent livor mortis of the dorsum, and early algor mortis. The hair is reddish brown and abundant, the eyes are blue, the right pupil measuring 8 mm. in diameter, the left 4 mm. There is edema and ecchymosis of the inner canthus region of the left eyelid measuring approximately 1.5 cm. in greatest diameter. There is edema and ecchymosis diffusely over the right supra-orbital ridge with abnormal mobility of the underlying bone. (The remainder of the scalp will be described with the skull.) There is clotted blood on the external ears but otherwise the ears, nares, and mouth are essentially unremarkable. The teeth are in excellent repair and there is some pallor of the oral mucous membrane.
Situated on the upper right posterior thorax just above the upper border of the scapula there is a 7 x 4 millimeter oval wound. This wound is measured to be 14 cm. from the tip of the right acromion process and 14 cm. below the tip of the right mastoid process.
Situated in the low anterior neck at approximately the level of the third and fourth tracheal rings is a 6.5 cm. long transverse wound with widely gaping irregular edges. (The depth and character of these wounds will be further described below.)
Situated on the anterior chest wall in the nipple line are bilateral 2 cm. long recent transverse surgical incisions into the subcutaneous tissue. The one on the left is situated 11 cm. cephalad to the nipple and the one on the right 8 cm. cephalad to the nipple. There is no hemorrhage or ecchymosis associated with these wounds. A similar clean wound measuring 2 cm. in length is situated on the antero-lateral aspect of the left mid arm. Situated on the antero-lateral aspect of each ankle is a recent 2 cm. transverse incision into the subcutaneous tissue.
There is an old well healed 8 cm. McBurney abdominal incision. Over the lumbar spine in the midline is an old, well healed 15 cm. scar. Situated on the upper antero-lateral aspect of the right thigh is an old, well healed 8 cm. scar.
Missile Wounds
1. There is a large irregular defect of the scalp and skull on the right involving chiefly the parietal bone but extending somewhat into the temporal and occipital regions. In this region there is an actual absence of scalp and bone producing a defect which measures approximately 13 cm. in greatest diameter.
From the irregular margins of the above scalp defect tears extend in stellate fashion into the more or less intact scalp as follows:
a. From the right inferior temporo-parietal margin anterior to the right ear to a point slightly above the tragus.
b. From the anterior parietal margin anteriorly on the forehead to approximately 4 cm. above the right orbital ridge.
c. From the left margin of the main defect across the midline antero-laterally for a distance of approximately 8 cm.
d. From the same starting point as c. 10 cm. postero-laterally.
Situated in the posterior scalp approximately 2.5 cm. laterally to the right and slightly above the external occipital protuberance is a lacerated wound measuring 15 x 6 mm. In the underlying bone is a corresponding wound through the skull which exhibits beveling of the margins of the bone when viewed from the inner aspect of the skull.
Clearly visible in the above described large skull defect and exuding from it is lacerated brain tissue which on close inspection proves to represent the major portion of the right cerebral hemisphere. At this point it is noted that the falx cerebri is extensively lacerated with disruption of the superior saggital sinus.
Upon reflecting the scalp multiple complete fracture lines are seen to radiate from both the large defect at the vertex and the smaller wound at the occiput. These vary greatly in length and direction, the longest measuring approximately 19 cm. These result in the production of numerous fragments which vary in size from a few millimeters to 10 cm. in greatest diameter.
The complexity of these fractures and the fragments thus produced tax satisfactory verbal description and are better appreciated in photographs and roentgenograms which are prepared.
The brain is removed and preserved for further study following formal in fixation.
Received as separate specimens from Dallas, Texas are three fragments of skull bone which in aggregate roughly approximate the dimensions of the large defect described above. At one angle of the largest of these fragments is a portion of the perimeter of a roughly circular wound presumably of exit which exhibits beveling of the outer aspect of the bone and is estimated to measure approximately 2.5 to 3.0 cm. in diameter. Roentgenograms of this fragment reveal minute particles of metal in the bone at this margin. Roentgenograms of the skull reveal multiple minute metallic fragments along a line corresponding with a line joining the above described small occipital wound and the right supra-orbital ridge. From the surface of the disrupted right cerebral cortex two small irregularly shaped fragments of metal are recovered. These measure 7 x 2 mm. and 3 x 1 mm. These are placed in the custody of Agents Francis X. O'Neill, Jr. and James W. Sibert, of the Federal Bureau of Investigation, who executed a receipt therefore (attached).
2. The second wound presumably of entry is that described above in the upper right posterior thorax. Beneath the skin there is ecchymosis of subcutaneous tissue and musculature. The missile path through the fascia and musculature cannot be easily proved. The wound presumably of exit was that described by Dr. Malcolm Perry of Dallas in the low anterior cervical region. When observed by Dr. Perry the wound measured "a few millimeters in diameter", however it was extended as a tracheostomy incision and thus its character is distorted at the time of autopsy. However there is considerable eccymosis of the strap muscles of the right side of the neck and of the fascia about the trachea adjacent to the line of the tracheostomy wound. The third point of reference in connecting these two wounds is in the apex (supra-clavicular portion) of the right pleural cavity. In this region there is contusion of the parietal pleura and of the extreme apical portion of the right upper lobe of the lung. In both instances the diameter of contusion and ecchymosis at the point of maximal involvement measures 5 cm. Both the visceral and parietal pleura are intact overlying these areas of trauma.
Incisions
The scalp wounds are extended in the coronal plane to examine the cranial content and the customary (Y) shaped incision is used to examine the body cavities.
Skeletal System
Aside from the above described skull wounds there are no significant gross skeletal abnormalities.
Photography
Black and white and color photographs depicting significant findings are exposed but not developed. These photographs were placed in the custody of Agent Roy E. Kellerman of the U.S. Secret Service, who executed a receipt therefore (attached).
Roentgenograms
Roentgenograms are made of the entire body and of the separately submitted three fragments of skull bone. These are developed are were placed in the custody of Agent Roy H. Kellerman of the U.S. Secret Service, who executed a receipt therefore (attached).
Summary
Based on the above observations it is our opinion that the deceased died as a result of two perforating gunshot wounds inflicted by high velocity projectiles fired by a person or persons unknown. The projectiles were fired from a point behind and somewhat above the level of the deceased. The observations and available information do not permit a satisfactory estimate as to the sequence of the two wounds.
The fatal missile entered the skull above and to the right of the external occipital protuberance. A portion of the projectile traversed the cranial cavity in a posterior-anterior direction (see lateral skull roentgenograms) depositing minute particles along its path. A portion of the projectile made its exit through the parietal bone on the right carrying with it portions of cerebrum, skull and scalp. The two wounds of the skull combined with the force of the missile produced extensive fragmentation of the skull, laceration of the superior saggital sinus, and of the right cerebral hemisphere.
The other missile entered the right superior posterior thorax above the scapula and traversed the soft tissues of the supra-scapular and the supra-clavicular portions of the base of the right side of the neck. This missile produced contusions of the right apical parietal pleura and of the apical portion of the right upper lobe of the lung. The missile contused the strap muscles of the right side of the neck, damaged the trachea and made its exit through the anterior surface of the neck. As far as can be ascertained this missile struck no bony structures in its path through the body.
In addition, it is our opinion that the wound of the skull produced such extensive damage to the brain as to preclude the possibility of the deceased surviving this injury.
A supplementary report will be submitted following more detailed examination of the brain and of microscopic sections. However, it is not anticipated that these examinations will materially alter the findings.
Supplementary Report of Autopsy Number A63-272 President John F. Kennedy
Pathological Examination Report No. A63-272
Gross Description of the Brain
Following formalin fixation the brain weighs 1500 gms. The right cerebral hemisphere is found to be markedly disrupted. There is a longitudinal laceration of the right hemisphere which is para-sagittal in position approximately 2.5 cm. to the right of the of the midline which extends from the tip of the occipital lobe posteriorly to the tip of the frontal lobe anteriorly. The base of the laceration is situated approximately 4.5 cm. below the vertex in the white matter. There is considerable loss of cortical substance above the base of the laceration, particularly in the parietal lobe. The margins of this laceration are at all points jagged and irregular, with additional lacerations extending in varying directions and for varying distances from the main laceration. In addition, there is a laceration of the corpus callosum extending from the genu to the tail. Exposed in this latter laceration are the interiors of the right lateral and third ventricles.
When viewed from the vertex the left cerebral hemisphere is intact. There is marked engorgement of meningeal blood vessels of the left temporal and frontal regions with considerable associated sub-arachnoid hemorrhage. The gyri and sulci over the left hemisphere are of essentially normal size and distribution. Those on the right are too fragmented and distorted for satisfactory description.
When viewed from the basilar aspect the disruption of the right cortex is again obvious. There is a longitudinal laceration of the mid-brain through the floor of the third ventricle just behind the optic chiasm and the mammillary bodies. This laceration partially communicates with an oblique 1.5 cm. tear through the left cerebral peduncle. There are irregular superficial lacerations over the basilar aspects of the left temporal and frontal lobes.
In the interest of preserving the specimen coronal sections are not made. The following sections are taken for microscopic examination:
a. From the margin of the laceration in the right parietal lobe.
b. From the margin of the laceration in the corpus callosum.
c. From the anterior portion of the laceration in the right frontal lobe.
d. From the contused left fronto-parietal cortex.
e. From the line of transection of the spinal cord.
f. From the right cerebellar cortex.
g. From the superficial laceration of the basilar aspect of the left temporal lobe.
During the course of this examination seven (7) black and white and six (6) color 4x5 inch negatives are exposed but not developed (the cassettes containing these negatives have been delivered by hand to Rear Admiral George W. Burkley, MC, USN, White House Physician).
Microscopic Examination
Brain
Multiple sections from representative areas as noted above are examined. All sections are essentially similar and show extensive disruption of brain tissue with associated hemorrhage. In none of the sections examined are there significant abnormalities other than those directly related to the recent trauma.
Skin Wounds
Sections through the wounds in the occipital and upper right posterior thoracic regions are essentially similar. In each there is loss of continuity of the epidermis with coagulation necrosis of the tissues at the wound margins. The scalp wound exhibits several small fragments of bone at its margins in the subcutaneous tissue.
Final Summary
This supplementary report covers in more detail the extensive degree of cerebral trauma in this case. However neither this portion of the examination nor the microscopic examinations alter the previously submitted report or add significant details to the cause of death.
/s/
J. J. HUMES
CDR, MC, USN, 497831
Missing and Botched Evidence
Key evidence such as crucial autopsy photos and even President Kennedy's brain went missing out of the National Archives. Their whereabouts is still unknown, which brings suspicion about a coverup in this investigation. Some believe Robert Kennedy requested the brain to be buried with his brother. However, no-one knows for certain what happened to John Kennedy's brain.
A witness at Kennedy's autopsy, Francis X. O'Neill Jr, recalled "there was not much of the brain left" and that "more than half of the brain was missing" when it was removed from Kennedy's skull and placed in a white jar. O'Neill was shocked when he was shown the official autopsy photos showing a brain that was much less damaged. "This looks almost like a complete brain", he said. A theory about a 'second brain' emerged as it was believed that this was a medical coverup to keep the evidence in check with the Lee Harvey Oswald shot to JFK's head.
The pathologist who carried out the autopsy did not have experience in gunshot wounds. He was told to just find the bullet believed to still be inside the President. The Kennedy family requested that a full-body autopsy was not to be carried out. For some reason Kennedy's head was not shaved in order to examine the gunshot closer, and so hair obscures the wound in the autopsy photos.
While Kennedy was in hospital, the tracheal tube used to keep him breathing was put through what may have been a gunshot hole in his throat, so there is no way to know if the hole shown in the photos was a gunshot wound made bigger for the tube, or purely just a medical incision.
A witness at Kennedy's autopsy, Francis X. O'Neill Jr, recalled "there was not much of the brain left" and that "more than half of the brain was missing" when it was removed from Kennedy's skull and placed in a white jar. O'Neill was shocked when he was shown the official autopsy photos showing a brain that was much less damaged. "This looks almost like a complete brain", he said. A theory about a 'second brain' emerged as it was believed that this was a medical coverup to keep the evidence in check with the Lee Harvey Oswald shot to JFK's head.
The pathologist who carried out the autopsy did not have experience in gunshot wounds. He was told to just find the bullet believed to still be inside the President. The Kennedy family requested that a full-body autopsy was not to be carried out. For some reason Kennedy's head was not shaved in order to examine the gunshot closer, and so hair obscures the wound in the autopsy photos.
While Kennedy was in hospital, the tracheal tube used to keep him breathing was put through what may have been a gunshot hole in his throat, so there is no way to know if the hole shown in the photos was a gunshot wound made bigger for the tube, or purely just a medical incision.
